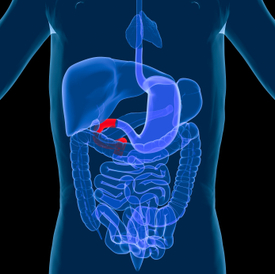
Hypertrophic pyloric stenosis (HPS) in infants is a narrowing of the pylorus, the lower part of the stomach through which food and other stomach contents pass to enter the small intestine. When an infant has HPS, the muscles in the pylorus have enlarged resulting in narrowing within the pyloric channel preventing food from emptying out of the stomach.
HPS is a form of gastric outlet obstruction, which means a blockage from the stomach to the intestines. It affects three out of every thousand babies born in the United States. It’s about four times more likely to occur in firstborn male infants and also has been shown to run in families. HPS occurs more commonly in Caucasian infants than in babies of other ethnic backgrounds.
Despite numerous hypotheses, the exact cause of HPS is not fully understood. It is believed that these babies are not born with it, but that the progressive thickening of the pylorus occurs after birth. A baby will start to show symptoms when the pylorus is so thickened that the stomach can no longer empty properly.
The thickening of the pyloric muscles may be a due to a combination of several factors. The use of erythromycin in the first 2 weeks of life has been associated with HPS, and there is also a connection in babies whose mothers took this antibiotic at the end of pregnancy or during breastfeeding.
Projectile vomitinforceful ejection of milk or formula up to several feet away, within 30 minutes after feeding. Vomiting may be mild at first and gradually become more severe. The vomit may sometimes contain blood. Babies are usually not ill-looking or febrile. In the early stage of the disease they remain hungry and suck vigorously after episodes of vomiting.
Persistent hunger– Babies often want to eat soon after vomiting
Stomach contractions– These are noticeable wave-like contractions that move across the upper abdomen (peristalsis) soon after feeding but before vomiting. This is caused by stomach muscles trying to force food past the outlet of the pylorus
Dehydration– prolonged delay in diagnosis can lead to dehydration. The infant with cry without tears or become lethargic. Diapers need to be changed less often and won’t be as wet as wet as they should be.
Changes in bowel movements– since food is prevented from reaching the intestines, babies with this condition may be constipated.
Weight problems– babies will not gain weight, and can sometimes even lose weight. Parents often report trying several different baby formulas because they (or their physicians) assume vomiting is due to intolerance.
There are other conditions that can resemble HPS, such as gastroesophageal reflux disease (GERD). This usually begins at eight weeks of age, with excess spitting up, or reflux, occurring after feedings. However, the majority of infants with GERD do not experience projectile vomiting, and although they may have poor weight gain, they tend to have normal stools.
In infants with gastroenteritis, which is an inflammation in the digestive tract that can be caused by viral or bacterial infection, their symptoms may also resemble HPS. Vomiting and dehydration are seen with both conditions; however, infants with gastroenteritis will often have diarrhea with loose, watery, or sometimes bloody stools. Diarrhea usually isn’t seen with HPS.
Once HPS is diagnosed, early consultation with a surgeon familiar with neonatal care is warranted because treatment is essentially surgical. This is especially important if the child requires transfer to another facility for surgical care. The American Pediatric Surgical Association offers guidelines for appropriate consultation and transfer of small infants. Good outcome has been shown to depend on the quality of preoperative correction of fluid and electrolyte abnormalities, availability of a pediatric anesthetist, and training level of the surgeon.
Pyloromyotomy, the surgical procedure in which an incision is made in the longitudinal and circular muscles of the pyloris is the procedure of choice. Laparoscopic pyloromyotomy has a significantly shorter recovery time compared with open pyloromyotomy. However, open pyloromyotomy has a higher efficacy and fewer complications. Endoscopic pyloromyotomy, another alternative, can be performed as an outpatient procedure. Recently, endoscopic balloon dilatation of HPS after failed pyloromyotomy has been used with greater frequency.