-
Posted by Dr. Jack Sacks on May 24, 2018.
The prevalence of brain injury in the United States is alarming as it is the second leading cause of disability in the country. Often referred to as the silent epidemic, approximately 3.17- 5.3 million Americans suffer from traumatic brain injuries, another 4.7 million have brain injuries from strokes, and another 500,000 have cerebral palsy (brain injury due to an event of oxygen deprivation). Causes of brain injury that may give rise to a medical malpractice lawsuit are further described below:
 Brain Injury from Birth: a medical malpractice lawsuit may arise may when a child’s brain is negligently deprived of oxygen during pregnancy, labor and delivery. This may result in the child later developing cerebral palsy, mental retardation, seizures, blindness, deafness, and learning disabilities. Oxygen deprivation that injures a baby’s brain may arise from any of the following events:
Brain Injury from Birth: a medical malpractice lawsuit may arise may when a child’s brain is negligently deprived of oxygen during pregnancy, labor and delivery. This may result in the child later developing cerebral palsy, mental retardation, seizures, blindness, deafness, and learning disabilities. Oxygen deprivation that injures a baby’s brain may arise from any of the following events:
*Compression of the umbilical cord during delivery
*Maternal Infection present during the pregnancy or delivery
*Placental abruption or uterine rupture prior to birth
*Maternal high blood pressure during the pregnancy (preclampsia)
*Breeched vaginal position of the baby (feet first rather than head first)
*Improper administration or doasage of epidural or labor inducing drugs during the delivery
*Failure to timely perform an emergency c-section
*Fetal macrosomia (oversized baby) unable to navigate the birth canal
Brain Injury in Adults and Children: a medical malpractice lawsuit may arise as a result of errors in diagnosis and treatment of a serious medical condition. A few of the causes of brain injury in children and adults that may involve medical malpractice include:
*Medication errors
*Anesthesia errors
*Surgical errors
*Radiology errors
*Emergency room errors
*Delay in diagnosis/treatment of heart attack or cardiac arrest
*Delay in diagnosis/treatment of a stroke, aneurysm, or blood clot
*Delay in diagnosis/treatment of meningitis or encephalitis
*Delay in diagnosis/treatment of a spreading infection or abscess
*Delay in diagnosis/treatment of internal bleeding
*Delay in diagnosis/treatment of hydrocephalus
*Delay in diagnosis/treatment of diabetes/diabetic coma/insulin shock
In addition to the above mentioned causes of brain injury, many other errors involving patient treatment and care may give rise to a lawsuit. One of the most common causes occurs when a hospital patient or nursing home patient falls (due to inadequate protective measures) and the patient suffers a traumatic brain injury. In fact, falls are the leading cause of traumatic brain injury in our country surpassing even motor vehicle accidents. For a detailed guide to the incidence, prevalence, and epidemiology of brain injury, seeEssential Brain Injury Guide prepared under the auspices of the Brain Injury Association of America.
Topic: Allergic Reactions, Aneurysm, Birth Injury, Brachial Plexus Injury, Brain Injury, Cerebral Palsy, Erb's Palsy, Failure to Diagnose, Falls/Fractures, Heart Attack, High Blood Pressure, Hydrocephalus, Hypogylcemia, Infection, Lumbar Puncture, Meningitis, Paralysis, Peritonitis, Premature Birth, Shoulder Dystocia, Spinal Injury, Spinal Tap, Stroke, Surgical Mistakes Comments Off on Brain Injury and Medical Malpractice
-
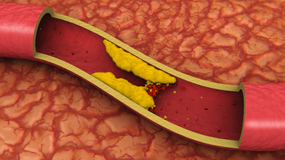
Deep venous thrombosis is the development of a blood clot in the large, deep veins of the lower leg and thigh. Thrombi can cause tissue injury due to vascular occlusion or distal embolization. However, venous obstruction can be offset by collateral blood vessels. Thrombi can also cause local pain and edema due to the blockage of blood flow. If the clot breaks off and travels through the blood, it is referred to as an embolism. An embolism can become trapped in the brain, lungs, or heart leading to major injury. Pulmonary embolus (PE) is a common complication and life threatening if not treated quickly with anticoagulants. PE presents with shortness of breath, chest pain, and cough with blood in sputum.
 DVT can occur with stasis or in hypercoaguable states. It is commonly seen following trauma, surgery, or burns, which contribute to decreased physical activity, damage to vessels, and release of procoagulant substances from tissues. Reduced physical activity causes a decline in the milking action of lower leg muscles and slows venous return. Risk factors for DVT include advanced age, bed rest, immobilization, smoking, birth control pills, family history of blood clots, fractures in the pelvis or legs, giving birth within the last 6 months, heart failure, and obesity. To prevent DVT, patients should move their legs during long flights or when they are immobile for long periods of time.
DVT can occur with stasis or in hypercoaguable states. It is commonly seen following trauma, surgery, or burns, which contribute to decreased physical activity, damage to vessels, and release of procoagulant substances from tissues. Reduced physical activity causes a decline in the milking action of lower leg muscles and slows venous return. Risk factors for DVT include advanced age, bed rest, immobilization, smoking, birth control pills, family history of blood clots, fractures in the pelvis or legs, giving birth within the last 6 months, heart failure, and obesity. To prevent DVT, patients should move their legs during long flights or when they are immobile for long periods of time.
Although many DVTs are asymptomatic, they can recur. Some individuals suffer from post-phlebitic syndrome, which involves chronic pain and swelling in the leg. The major symptoms of DVT include changes in a patient’s leg such as redness, increased temperature, pain, and tenderness. Diagnosis is based on the physical exam, which should demonstrate a red, swollen leg. Diagnostic tests include a D-dimer blood test along with other blood tests to check for hypercoagulability such as activated protein C resistance, anti-thrombin III levels, antiphospholipid antibodies, and genetic testing for mutations with a predisposition towards blood clots. Imaging studies of the legs include Doppler ultrasound, plethysmography, and radiography.
The primary treatment for DVT is anti-coagulants, also known as blood thinners. They prevent the formation of new clots and the growth of old clots. However, they cannot dissolve existing clots. Patients are more likely to bleed on these medications. Heparin is an IV administered anticoagulant given in a hospital setting. Warfarin (Coumadin) is an oral anticoagulant that takes several days to work; thus, Heparin cannot be stopped until Warfarin is functioning at an effective dose for a minimum of two days. Many patients wear pressure stockings on their legs to improve blood flow and decrease their risk of DVT. When medications are ineffective, patients may need to undergo surgery. A filter can be placed in the body’s largest vein to prevent thrombi from migrating to the lungs. Also, surgery may be necessary to remove large thrombi.
Topic: Amputations, Brain Injury, Deep Venous Thrombosis, Failure to Diagnose, Heart Attack, Paralysis, Pulmonary Embolism, Stroke Comments Off on Deep Venous Thrombosis and Medical Malpractice
-
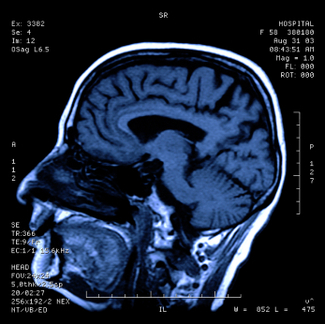
One of the first steps in evaluating brain injury is diagnostic imaging. Imaging refers to various methods of viewing the structures and processes residing in the brain. Some of the more familiar modalities are CT (or CAT) scans, which use X-rays to evaluate intracranial structures. MRI, Magnetic Resonance Imaging, uses magnetic fields to illustrate the brain. However, in cases of traumatic brain injury (TBI), more advanced methods may be needed for proper diagnosis.
An MRI machine can use special software to perform a brain scan called Diffusion Tensor Imaging (DTI). This scan detects the diffusion of water across brain cells and highlights certain areas that may be associated with injury. These injuries may not be apparent on conventional MRI’s.
PET scan (Positron Emission Tomography) measures uptake and metabolism of glucose from a small radioactive “tagged” sample injected into the patient. The scanner monitors this sample as the brain utilizes it. The metabolic uptake and usage may differ in patients who have suffered a brain injury. This helps define the extent and type of injury.
In SPECT (Single Photon Emission Computed Tomography), the tagged sample is not absorbed or utilized in the brain cells. Instead, it remains in the blood stream and demonstrates the blood movement or perfusion through the brain. Areas of brain injury or damage may not have normal blood flow so the SPECT scan helps define these areas.
Brain injuries can result from medical malpractice. A baby may suffer birth trauma during labor and delivery. A child may have a concussion or sports injury misdiagnosed or improperly evaluated by a physician. An individual injured in a car accident may not have the indicated testing done by the emergency room. Although scientific progress in imaging studies has improved the ability to diagnose and evaluate brain injuries, these tests need to be utilized in the appropriate situations so patient results and outcomes can improve.
Topic: Aneurysm, Birth Injury, Brain Injury, Failure to Diagnose, Falls/Fractures, High Blood Pressure, Hydrocephalus, Infection, Lumbar Puncture, Meningitis, Paralysis, Placental Abruption, Spinal Injury, Spinal Tap, Stroke Comments Off on Advanced Diagnostic Imaging for Acquired Brain Injury
-
Child neglect is the most prevalent form of child maltreatment in the US. According to the National Child Abuse and Neglect Data System (NCANDS), approximately 899,000 children in the US who were victims of abuse and neglect in 2005, 62.8% suffered from neglect alone. Child neglect is a failure by parents or caregivers to provide for a child’s basic physical, educational, and emotional needs. It is difficult to define because it varies with the age and development of the child; therefore, it is problematic to determine the extent of the problem. Risk factors for abuse include: preexisting mental or physical illness, poverty, familial stress, substance abuse by parents or caregives. Physicians, nurses, day care personnel, relatives, and neighbors are generally the ones to suspect and report neglect; however, they may be the culprits too. Often times, signs of child neglect may include inadequate medical or custodial care.
Physical neglect encompasses the majority of neglect cases and it involves the parent/caretaker not granting the child basic necessities such as food, clothing, medical care, and shelter. By depriving the child of these essential things, his or her physical health, well being, psychological growth and development is jeopardized. Failure to thrive, malnutrition, serious illness, physical injury due to lack of supervision, and low self-esteem are a some of the byproducts of physical neglect. As an unfortunate example, infants are sometimes mistakenly left behind in cars or vans by their caregivers when the outside temperature is very hot, resulting in heat stroke or death to these infants.
Regarding child abuse, medical neglect is the failure to deliver necessary healthcare for a child thereby endangering the child’s well being. Situations involving medical neglect include when a parent refuses medical care for a child in an emergency or when a parents does not follow recommendations for a child with a treatable chronic disease or disability. Medical neglect often correlates with poverty; however, there is a difference between an inability to provide the appropriate care due to finances or cultural norms and being purposefully neglectful.
If one suspects child neglect, the first step is to report the incident to local child protective services agency in the county or state. The majority of states have a child abuse hotline or you can use the Childhelp National Child Abuse Hotline (1-800-4-A-CHILD). Professionals involved with children have a duty to report reasonable suspicion of abuse and neglect. Reasonable suspicion is based on objective evidence which includes firsthand observation or statements made by a parent or child. Symptoms of negelect include: difficulties in school, eating disorders, low self esteem, depression, anxiety, signs of physical injury, rebellious behavior, sleep disorders, and other vague physical complaints.
Topic: Birth Injury, Child Abuse, Child Neglect, Stroke Comments Off on Child Abuse and Neglect
-
An outbreak of fungal meningitis due to contaminated epidural methylpredinsolone (steroid) injections, made by the New England Compounding Center, has been ongoing throughout the United States. Meningitis is a disease caused by inflammation of the meninges, the membranes that cover the brain and spinal cord. It can be caused by bacteria, viruses, fungus, physical injury, cancer, and certain medications. Fungal meningitis is generally rare and non-contagious. In the recent outbreak of fungal meningitis, the contaminant was an environmental mold known as Exerohilum rostratum, a plant pathogen that rarely causes human disease. It was identified by polymerase chain reaction assay from CSF in at least 25 patients and it has been detected in at least one unopened vial from the implicated batch of methylprednisolone . A quarter of the steroid vials in a bin at the England Compounding center contained “greenish black foreign matter” and several rooms utilized to produce sterile products demonstrated mold or bacterial overgrowth according to the FDA.
All locations that received contaminated injections were notified and individuals who received injections from these locations were informed of the possibility of fungal infection. It is likely that not every individual who underwent an injection will contract fungal meningitis. However, individuals with underlying health conditions, circumstances surrounding the injection, and the level of contamination of a particular vial may increase susceptibility. The New England compounding center, where the injections were produced, was closed and all their products were recalled. The CDC currently reports over 300 infected and 25 deaths in patients who received contaminated injections.
Patients should inform physicians of any symptoms such as new-onset headache, neck stiffness, photophobia, fever, or a stroke-like presentation. The incubation period is 1-4 weeks after receiving the contaminated injection. Any individual can contract fungal meningitis; however, it is often seen in individuals with weakened immune systems, such as AIDs or cancer, or individuals taking immune-suppressants, like steroids or anti-TNF medications.
Blood cultures, imaging (Xray or CT), and lumbar puncture are used to diagnose meningitis. A definitive diagnosis is generally made by evaluating cerebrospinal fluid collected from a lumber puncture, also known as a spinal tap. CSF findings in fungal meningitis are increased pressure, increased protein, decreased glucose, and increased lymphocytes. It is essential to diagnose the specific cause of meningitis to determine treatment and severity of illness. Fungal meningitis is generally treated with long courses of high dose intravenous antifungal medications, such as amphotericin B or flucytosine. The length of treatment depends on the patient’s immune status and type of fungus. Individuals with weakened immune systems need to remain on treatment for longer.
Topic: Brain Injury, Epidural, Lumbar Puncture, Meningitis, Products Liability, Stroke Comments Off on Fungal Meningitis Outbreak- over 300 infected, 25 deaths
-
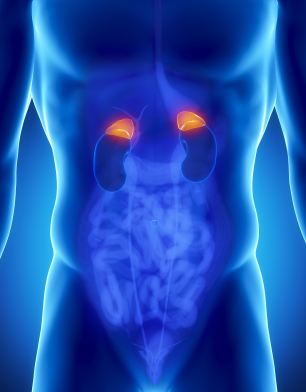
Pheochromocytoma is an adrenal gland tumor comprised of chromaffin cells that produce and release excess epinephrine and norepinephrine, which are hormones that effect heart rate, metabolism, and blood pressure. Pheochromocytomas are generally benign and can appear at any age; however, they commonly occur during middle age.
If left untreated or unrecognized, this tumor can be life threatening. Researchers have yet to discover the underlying cause of pheochromocytoma. However, certain disorders such as Multiple Endocrine Neoplasia type II (MEN II), Von Hippel Lindau disease, Neurofibromatosis 1, and Familial Paraganglioma are associated with pheochromocytoma.
Isolated, paroxysmal episodes of hypertension occur in fewer than half of individuals with pheochromocytoma. Episodes of hypertension can occur at unpredictable intervals and usually last 15-20 minutes. During these episodes, the patient experiences hypertension, tachycardia, and fever; however, the patient’s vital signs can be normal at other times. As the tumor grows, episodes increase in frequency, length, and severity. Additional symptoms include abdominal pain, chest pain, irritability, pallor, and weight loss.
However, two thirds of patients experience chronic sustained hypertension. Whether sustained or episodic, the patient’s hypertension is associated with an increased risk of myocardial ischemia, heart failure, renal injury, and cerebrovascular accidents. Sudden cardiac death may occur secondary to catecholamaine-induced myocardial irritability and ventricular arrhythmias.
Diagnosis of pheochromocytoma is based on elevated levels of free catecholamines and metabolites, such as vanillymandelic acid and metanephrines, in the patient’s urine. The following additional tests can be used to diagnose pheochromocytoma: abdominal CT scan, adrenal biopsy, catecholamines blood test, glucose blood test, metanephrine blood test, MIBG scintiscan, and MRI of the abdomen.
The current treatment for pheochromocytoma is surgery to excise the tumor. It is essential to stabilize the patient’s blood pressure and pulse with adrenergic blocking medication prior to surgery. When the tumor cannot be removed, medication is required to manage it. The majority of patients have benign tumors that are excisable; however, 10% of tumors recur and 25% of patients still have high blood pressure after surgery.
A medical malpractice lawsuit may arise when a patient presents with typical signs and symptoms of pheochromocytoma but the doctor fails to make the diagnosis thereby causing bodily injury, disability or death to the patient usually as a result of uncontrolled hypertension.
Topic: Adrenal Gland, Heart Attack, High Blood Pressure, Pheochromocytoma, Stroke Comments Off on Pheochromocytoma and Medical Malpractice
-
A pituitary adenoma is generally a benign, slow growing tumor that occurs in the pituitary gland. The pituitary gland is a small, bean shaped structure that lies at the base of the brain. It has a central role in the regulation of hormones that affect the body such as Adrenocorticotropic hormone (ACTH), Growth hormone (GH), Prolactin, and Thyroid-stimulating hormone (TSH).
Approximately 1 in 1,000 individuals have pituitary adenomas. They are generally not cancerous but may invade nearby structures. They are classified based on size. A microadenoma is less than 1 cm in diameter whereas a macroadenoma is larger than 1 cm in size.
Based on whether the pituitary adenoma is a hormone-producing or hormone-inactive tumor, the patient will present with different symptoms. Hormone-producing tumors will make excessive amounts of an active hormone so symptoms present as a hormonal imbalance. The three most common hormone-producing adenomas are Prolactinomas, Growth hormone-secreting pituitary adenoma, and ACTH-secreting pituitary adenoma.
If the patient has a large hormone-inactive or hormone-producing tumor, it may compress surrounding brain structures due to its size. Large pituitary tumors may compress the pituitary gland contributing to pituitary failure, which can lead to sexual dysfunction, inadequate body cortisol levels, and hypothyroidism. Other possible presentations relating to compression of brain structures include visual loss, headache, the “stalk effect”, and pituitary apoplexy. The “stalk effect” is due to the compression of the pituitary stalk, the structure connecting the brain to the pituitary gland, which leads to a mild elevation in the hormone prolactin. Higher levels of prolactin in females can contribute to irregular menstrual cycles. Pituitary apoplexy presents with an abrupt headache and visual loss. It can occur under two different situations. The pituitary adenoma can bleed internally causing a sudden increase in size or the tumor can outgrow its blood supply and the dead tissue will swell.
Pituitary adenomas can be diagnosed based on endocrine function testing, imaging, and visual field testing. Often times, visual problems may be the only symptom present. Optometrists and ophthalmologists should seriously consider the possibility of a pituitary tumor when the patient presents with an unexplained loss of visual field (especially peripheral vision), double vision, or blurred vision as the growth of a pituitary tumor can cause compression on the visual pathway (retina, optic nerve, etc). A delay in diagnosis of a pituitary adenoma may result in permanent loss of vision due to the damage caused by this compression. Endocrine function testing evaluates cortisol, follicle-stimulating hormone, lutenizing hormone, insulin growth factor-1, prolactin, testosterone/estradiol, and thyroid hormone levels. The preferred method of imaging is MRI, which screens for adenomas larger than 4 mm.
Treatment for pituitary adenomas depends on the presence of hormone production, size of the tumor, invasion of the tumor into surrounding structures, and the age and health of the patient. Drug therapy is used to treat hormone-producing tumors. For example, bromocriptine and cabergoline are used to treat tumors secreting prolactin because these medications decrease prolactin levels and tumor size. Pituitary adenomas that require surgery are usually minimally invasive techniques, where the tumor is removed through the nose. On the other hand, radiation therapy involves high doses of radiation being delivered to the tumor. It is a treatment utilized for pituitary adenomas that cannot be controlled by drug therapy or surgical intervention. Patients have the best outlook when the entire tumor can be removed.
Topic: Birth Injury, Brain Injury, Brain Tumor, Failure to Diagnose, Hydrocephalus, Paralysis, Pituitary Adenoma, Radiation Injury, Stroke, Surgical Mistakes Comments Off on Pituitary Adenomas and Medical Malpractice
-
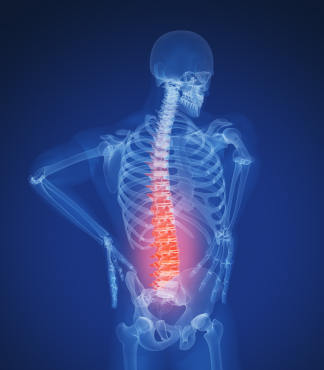
Lumbar puncture is a procedure performed in the lower back area, where a needle is inserted between two vertebrae to remove a sample of cerebrospinal fluid (CSF). The patient flexes his/her back to widen the spaces between the vertebrae so it is easier for the physician to access the region. The back is washed with antiseptic soap or iodine and covered with a sterile sheet. A local anesthetic is used to numb the area and then a thin hollow needle is inserted through the spinal membrane and into the spinal canal. During this portion of the procedure, the patient generally feels pressure. The CSF pressure is measured, a small amount of fluid is removed, and the pressure is measured again. The needle is removed and the site is bandaged. The total procedure takes about 45 minutes.
Lumbar puncture is used to collect CSF for analysis to help in diagnosing conditions such as subarachnoid hemorrhage (typically caused by ruptured aneurysm or traumatic brain injury), meningitis (inflammation of the membranes around the brain), and cancers of the brain or spinal cord. Lumbar Puncture may also be utilized to inject anesthetic medications, chemotherapeutic drugs, contrast material, or radioactive substances into CSF.
Lumbar Puncture may be used to identify increased or decreased CSF pressure. Increased CSF pressure can be caused by increased intracranial pressure as is seen with traumatic brain injury, ruptured aneurysm, and sometimes hydrocephalus. On the other hand, decreased CSF pressure can be caused by spinal cord tumor, shock, fainting, or diabetic coma. Normal CSF appears clear and colorless. When an infection is present, the CSF may look cloudy and be yellow or pink in color. Infection may be suspected if there is an increased level of white blood cells and/or protein. Increased CSF glucose indicates hyperglycemia whereas decreased CSF glucose may reflect hypoglycemia, bacterial or fungal infection, tuberculosis, or meningitis. If tumor cells are detected, the patient may have cancer in the brain, spinal cord, or CSF. If there are increased gamma globulin levels, the patient may be suffering from multiple sclerosis, neurosyphilis, or Guillan-Barre syndrome. The analysis of the CSF by the lab and the measuring of CSF pressure recorded from the lumbar puncture help in determining a diagnosis in many serious clinical situations.
Topic: Aneurysm, Brain Injury, Diabetes, Failure to Diagnose, Falls/Fractures, High Blood Pressure, Hydrocephalus, Hypogylcemia, Infection, Lumbar Puncture, Meningitis, Paralysis, Spinal Injury, Spinal Tap, Stroke Comments Off on Lumbar Puncture – Indications and Usage
-
A ventricular septal defect (VSD) refers to a hole in the ventricular septum, the wall dividing the left and right ventricles of the heart. VSDs are the most common congenital cardiac anomalies. They are found in30-60% of all newborns with a congenital heart defect, or about 2-6 per 1000 births. During heart formation, when the heart begins life as a hollow tube, it begins to partition, forming a septa. If this does not occur properly it can lead to an opening being left within the ventricular septum.
As noted above, during ventricular contraction some of the blood from the left ventricle is forced into the right ventricle from where it enters the lungs through the pulmonary arteries and then reenters the left ventricle via the pulmonary veins and left atrium. This refluxing of blood causes volume overload on the left ventricle. This increased blood volume also increases pressure in the right venticle eventually causing pulmonary hypertension with its associated symptoms. This effect is more noticeable in those with larger defects, who may present with shortness of breath, poor feeding and failure to thrive in infancy.
Because structural cardiac anomalies are estimated to occur in 8 of every 1,000 live births, it is imperative they be discovered before birth. Cardiovascular anomalies, such as VSD, are frequently associated with other congenital anomalies because the heart is among the last organs to develop completely in the embryo. The guidelines for routine prenatal evaluation of both the American College of Radiology and the American Institute of Ultrasound in Medicine require evaluation of the fetal heart. To not do so, may be consistent with medical negligence or medical malpractice.
The ultrasound view that is most commonly used is the four-chamber view of the heart. This allows for the assessment of abnormalities involving both right and left ventricles. Normally, both ventricles are approximately the same size. The left ventricle is posterior and to the left of the right ventricle. The wall between them, known as the interventricular septum separates the right ventricle from the left ventricle. A normal septum goes from the cardiac apex to the atrial septum. Formation of the interventricular septum begins at approximately 28 days gestation. A VSD results from maldevelopment of the embryonic septum.
A large VSD is easily diagnosed on the four-chamber view alone. However, color Doppler ultrasonography may be needed to demonstrate smaller defects, and some really small defects may not be detected until after birth. However, most of these close spontaneously. Fetal position is a major factor in the detection of VSD. For accurate diagnosis, it is critical that the ultrasound technician positions the transducer so the ultrasound beam is correctly directed relative to the septum. Not only can a VSD be missed, but a pseudo-VSD may result if performed incorrectly.
A small ventricular septal defect may never cause any problems. Larger defects can cause a wide range of disabilities, from mild to life-threatening. If pulmonary hypertension develops due to a large ventricular septal defect that goes untreated, over time, permanent damage to the lung arteries develops and the pulmonary hypertension becomes irreversible. This complication is known as Eisenmenger’s syndrome, and may occur in early childhood, or it can develop slowly over many years. Other complications that occur are heart failure, endocarditis, stroke, and heart arrhythmias which can lead to fatal complications. Becoming pregnant is also of concern due to the additional risks of pregnancy to women with VSDs undetected before birth and throughout childhood.
Though no treatment is necessary for small VSDs, larger VSDs demand certain precautions be taken, often with the baby being born in a tertiary care center and directly placed into the care of a pediatric cardiologist to determine if medical or surgical therapy is necessary to prevent the complications that will occur. That is why it is imperative that the diagnosis of VSD be made prior to birth.
Topic: Birth Injury, Failure to Diagnose, Heart Defect, Persistent Pulmonary Hypertension - Newborn, Stroke, Ventricular Septal Defect - Newborns Comments Off on Ventricular Septal Defect in the Newborn