Breast cancer affects millions of women in America and some studies indicate up to one out of eight women will be diagnosed with breast cancer over the course of her lifetime. The survival rate of breast cancer that is detected and treated early is much better than when a malignant tumor is found after it hasalready spread to lymph nodes or surrounding tissue. Therefore, it is important that every effort be made to diagnose and treat breast lesions as quickly as possible.
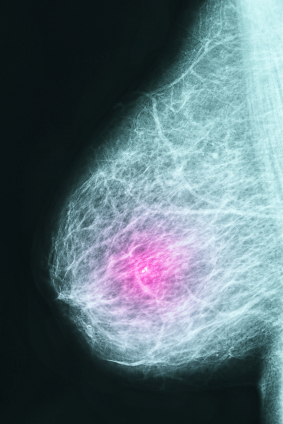
One of the mainstays in breast cancer detection is mammography. A mammogram involves an X-ray taken of the breasts, usually taken from several angles. Some abnormalities on mammograms such as masses or calcifications can alert the healthcare provider and patient that additional diagnostic testing needs to be done. The mammogram is one of the main methods of screening for breast cancer. Other imaging methods are less commonly used for screening, such as sonography (ultrasound), and MRI. However, these diagnostic methods can be used to add to information already obtained from a mammogram study when a patient is evaluated and uncertainty or an abnormality exists.
Patients need to be informed about the need for breast cancer screening. The mammogram, ultrasound, or MRI tests need to be read and interpreted correctly in order to diagnose problems and treat them early. In the case of breast cancer, early detection and diagnosis is key to improved cure rates. Special circumstances and risk factors (such as family history) may point to additional diagnostic testing to help identify breast cancer in those women at high risk. If tests are not interpreted correctly, or the results are not acted on in a timely or proper fashion by the healthcare provider, medical malpractice may be the result.
Sometimes patients or healthcare providers feel a breast mass or lump on examination. This often requires further evaluation usually beyond just a “regular” screening mammogram. As noted above, additional mammogram views, ultrasound, and/or MRI can help characterize the type of mass. However, breast masses usually warrant a visit to a surgeon or breast specialist to evaluate the patient for biopsy. Breast biopsies can be much less invasive to patients than in years past. During a “stereotactic” breast biopsy, the doctor employs mammography to locate the specific abnormal area and then a special instrument is used to remove cells from that precise area. Ultrasound can also be used to identify an abnormal area that is then biopsied. These methods are particularly useful when a breast mass cannot be felt. Sometimes when a mass can be felt, or palpated, the biopsy can be done without using X-ray or ultrasound localization.
Breast cancer screening can help identify women with breast cancer, as well as pre-cancerous lesions and benign breast conditions. Medical malpractice may occur as a consequence of failure to adequately evaluate, identify, screen, or diagnose breast cancer. Allegations of medical malpractice may include a failure by the internist to refer the patient to a breast specialist or surgeon for evaluation, failure by the radiologist to properly read a mammogram, ultrasound, or MRI, and/or failure by the pathologist to detect cancer in a breast biopsy that is indeed malignant. With improved methods of screening, diagnosis, and treatment of breast cancer, survival rates should continue to improve.